Your Diagnosis, Your Power
The more you know about how diagnoses are made, the more control you have over your mental health journey. Knowledge here = power in the doctor’s office.
Have you ever wondered how a practitioner decides if you’re struggling with depression, PTSD, or ADHD?
These diagnoses don’t come out of thin air—they’re guided by a single book that has shaped the way we understand mental health for decades. More than just a manual, the DSM-5 TR is the rulebook that influences everything from who gets treatment to what insurance will cover.
Love it or hate it, this book holds incredible power—and knowing how diagnoses are made gives you the chance to take control of your care by understanding the factors that shape them.
Don’t Just Get Diagnosed—Understand It
A diagnosis can determine your treatment, your options, and even your future. Understanding the DSM-5 TR (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) gives you a real seat at the table.
The DSM-5 TR (is the primary guide mental health professionals use to identify and diagnose conditions such as depression, anxiety, bipolar disorder, and ADHD.
Alongside it, clinicians also rely on the ICD-10 (International Classification of Diseases, Tenth Edition), a global system maintained by the World Health Organization that assigns standardized codes for all medical conditions, including mental health. These codes are essential for insurance, medical records, and ensuring consistency worldwide.
Here’s how a diagnosis of depression is defined in both the DSM-5 TR and the ICD-10:
- DSM-5 TR Official Label:
Major Depressive Disorder (MDD)
Can be specified as: mild, moderate, severe, with psychotic features, with seasonal pattern, with anxious distress, etc.
- ICD-10 Codes:
F32.x → Depressive episode
By using DSM-5 TR criteria together with ICD-10 codes, providers ensure that mental health diagnoses are consistent, evidence-based, and internationally recognized.
You can view the DSM-5 TR as a language used between Insurance companies, practitioners and patients that allow everyone to be on the same page. It allows a person to move between practitioners easily because the diagnostic criteria is widely understood and accepted.
But how did these systems come to be, and why are they so influential today? To answer that, we need to look at the history of the DSM and how it has evolved over time.

The History of the DSM: From DSM-I to DSM-5 TR
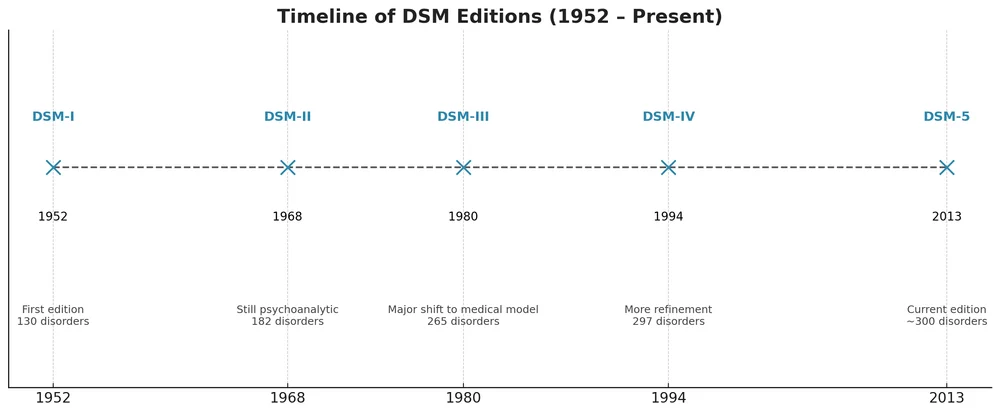
The DSM wasn’t always as detailed as it is today. The first edition, DSM-I, appeared in 1952, primarily to help clinicians standardize diagnoses in the post-World War II era. Over the decades, the DSM evolved through multiple revisions, each reflecting new scientific findings, changing societal attitudes, and advances in mental health care.
- DSM-I & DSM-II: Focused on expert consensus and descriptive.
- DSM-III: Introduced research-driven criteria and the multi-axial system.
- DSM-IV & DSM-IV-TR: Expanded cultural considerations and refined diagnostic categories.
- DSM-5 TR (2013): Integrated neuroscience, genetics, and a dimensional approach, removing the old multi-axial system.
As you can see, the DSM is an ever growing resource that changes alongside research and clinical practice. Experts don’t always agree on whether these changes truly reflect what happens in everyday clinical practice—or what most practitioners and the public believe. In this article, we’ll give a general overview of the DSM and also dig into some of these debates.
First, let’s start with a quick overview of what the DSM is and how it’s used in diagnosing mental health conditions.
The Purpose of the DSM-5 TR and ICD-10 in Mental Health
So why do clinicians rely on these manuals? Simply put, they serve several overlapping purposes:
- Diagnostic Standardization: DSM-5 TR criteria and ICD-10 codes help ensure that mental health diagnoses are accurate, consistent, and comparable across clinicians and settings.
- Communication: Both manuals provide a common language for clinicians, researchers, and educators, making it easier to discuss and study mental health conditions.
- Research Support: By standardizing definitions, these systems allow studies to reliably compare conditions, treatment outcomes, and population data.
- Insurance and Billing: ICD-10 codes are often required for coverage, linking diagnoses to payment systems and ensuring that patients receive appropriate care.
While the ICD-10 provides the coding framework, most diagnoses used in clinical practice are derived directly from the DSM-5 TR. This is why the DSM-5 TR is often considered the cornerstone of mental health evaluation—it guides not just treatment, but also research, education, and insurance documentation.

How the DSM-5 TR Was Created: Research, Experts, and Public Input
The DSM-5 TR was the result of 14 years of collaboration.
- A Task Force organized by the American Psychiatric Association led the project.
- 13 Work Groups of experts focused on categories like mood disorders, anxiety, and developmental conditions.
- Research from neuroscience, genetics, and epidemiology informed updates.
- For the first time, drafts were opened for public comment, adding transparency.
Takeaway: The DSM-5 TR is both a scientific document and a cultural one—it reflects research findings as well as social and professional input.
The Purpose of the DSM-5 TR in Mental Health Diagnosis
The DSM-5 TR has four key purposes:
- Diagnostic Standardization – Clear criteria for identifying mental health disorders.
- Communication – A common language for clinicians, researchers, and educators.
- Research – Provides consistent categories for scientific studies.
- Insurance and Reimbursement – Used by insurance companies to determine coverage.
How Clinicians Use the DSM-5 TR in Practice
The DSM-5 TR doesn’t tell clinicians how to treat, but it does tell them what they’re treating.
Example: A diagnosis of Major Depressive Disorder requires at least five symptoms—such as persistent sadness, loss of interest, or changes in sleep—lasting at least two weeks. Without the DSM-5 TR’s criteria, diagnoses could vary significantly between providers.
Benefits of the DSM-5 TR for Patients and Professionals
Clarity and Consistency – Reduces guesswork and standardizes diagnosis.
Better Communication – Ensures professionals across fields can collaborate effectively.
Supports Research – Provides clear definitions that make studies stronger.
Guides Treatment – While not a treatment manual, it informs clinical decision-making.
Callout Box: Think of the DSM-5 TR like a GPS—it doesn’t drive the car for you, but it shows you the map.

Criticisms of the DSM-5 TR: Where It Misses the Mark
Like any tool, the DSM-5 TR isn’t perfect—and plenty of experts (and patients) have pointed that out. Here are some of the main concerns:
Turning “Normal” into “Pathology”
Grief is a good example- it can include:
- Persistent sadness
- Changes in sleep or appetite
- Feelings of worthlessness
- Difficulty functioning in daily life
In previous editions of the DSM, depression was only diagnosed if these symptoms continued two months after a loss. This was referred to as “bereavement clause”. However, the DSM-5 TR removed this clause. The results are that, even just a few weeks after a loss—a doctor might diagnose Major Depressive Disorder (MDD).
This shift has pros and cons. On one hand, people who develop serious depressive symptoms after a loss may receive help sooner. On the other hand, it raises an important question: are we medicalizing normal human suffering, labeling a natural grieving process as a mental disorder simply because it is painful?
Note: The DSM-5 TR does address grief specifically when it is prolonged with the Diagnosis of Grief Disorder.

Overlapping Categories Can Blur the Lines
Ever felt like you could check boxes for both anxiety and depression? You’re not alone. Symptoms often overlap, making it hard to tell where one disorder ends and another begins. For example:
- Someone might experience persistent worry, restlessness, and difficulty concentrating (typical of anxiety) while also feeling hopeless, fatigued, and uninterested in activities (typical of depression).
- A teenager could feel socially anxious at school but also struggle with low mood and irritability at home, fitting criteria for both social anxiety and depressive symptoms.
- An adult might have panic attacks or heightened stress responses while also experiencing chronic fatigue and trouble sleeping, making it unclear whether the primary issue is anxiety, depression, or both.
These overlaps can make DSM-5 TR diagnoses feel less precise and more complex. Patients often want a clear explanation of what’s happening and a treatment plan that addresses the full picture, not just isolated symptoms.
Reflection Question: Have you ever felt like a diagnosis didn’t quite “fit” your lived experience? This is one of the main criticisms of the DSM-5 TR—it doesn’t always capture the full human story.
Cultural Bias: Does It Reflect All Experiences?
Another criticism is that the DSM-5 TR may not fully capture cultural differences in how symptoms appear. For example, anxiety may show up as physical symptoms like headaches or stomach pain in some cultures, rather than as emotional symptoms in others.
This raises an important question: are clinicians sometimes diagnosing through a Western lens, which may not match a person’s lived reality?
Why the DSM-5 TR Still Matters
Despite these criticisms, the DSM-5 TR remains the gold standard for mental health diagnosis worldwide. It provides structure, a common language, supports research, and helps patients access treatment.
Key Insight: The DSM-5 TR is a tool, not a definition of who you are.

Final Thought
The DSM-5 TR reminds us that diagnosing the mind is both an art and a science. Knowing its strengths and weaknesses lets us navigate mental health thoughtfully—while never forgetting that every person’s experience is unique.
Primary Sources
- DSM-5 TR-TR (Text Revision) — American Psychiatric Association, 2022.
- DSM-5 TR — American Psychiatric Association, 2013.
- Earlier editions for historical comparison: DSM-IV-TR (2000), DSM-IV (1994), DSM-III (1980), DSM-II (1968), DSM-I (1952).
Official Organizations
- American Psychiatric Association (APA)
- DSM resources: https://psychiatry.org/psychiatrists/practice/dsm
- National Institute of Mental Health (NIMH)
- Research on DSM categories and the RDoC framework: https://www.nimh.nih.gov
- World Health Organization (WHO)
- ICD-11 for comparison with DSM: https://icd.who.int
Key Resources on DSM-5 TR Updates and Critiques
1. Major Depressive Disorder in DSM-5 TR: Implications for Clinical Practice and Research of Changes from DSM-IV
- Authors: Rudolf Uher, Jennifer L. Payne, Barbara Pavlova, Roy H. Perlis
- Published: June 2014 in Depression and Anxiety
- Summary: This review examines significant changes in the diagnostic criteria for Major Depressive Disorder (MDD) from DSM-IV to DSM-5 TR TR, including the removal of the bereavement exclusion, the introduction of new specifiers, and the reclassification of dysthymia as Persistent Depressive Disorder. The authors discuss the implications of these changes for clinical practice and research.
- Access: Available on PubMed and Wiley Online Library
2. Saving Normal: An Insider’s Revolt Against Out-of-Control Psychiatric Diagnosis
- Author: Allen Frances
- Published: 2013
- Summary: In this book, Allen Frances, former chair of the DSM-IV Task Force, critiques the expansion of psychiatric diagnoses in DSM-5 TR, arguing that it leads to the medicalization of normal human experiences. He discusses the implications of these changes for both patients and clinicians.
3. The Book of Woe: The DSM and the Unmaking of Psychiatry
- Author: Gary Greenberg
- Published: 2013
- Summary: Gary Greenberg offers an in-depth look at the creation of DSM-5 TR, providing insights into the controversies and debates that shaped its development. He explores the impact of the DSM on the field of psychiatry and the lives of patients.