Antidepressants are medicines used to treat depression, anxiety, and other mental health conditions. Two of the most common types are SSRIs (Selective Serotonin Reuptake Inhibitors) and SNRIs (Serotonin–Norepinephrine Reuptake Inhibitors).*
Callout Box: What a Reuptake Inhibitor Does
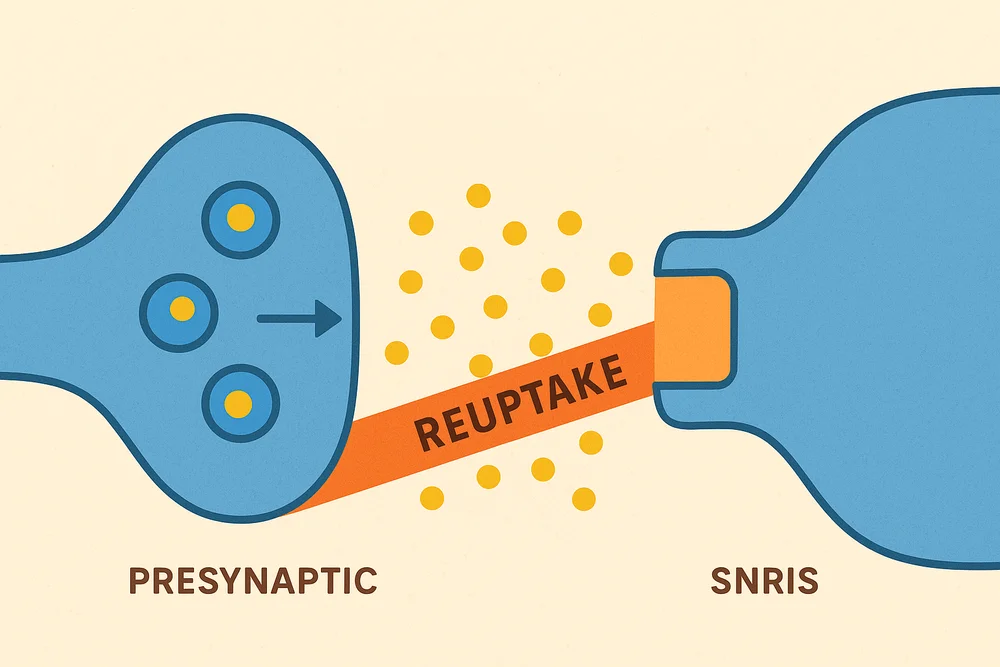
Both SSRIs and SNRIs are reuptake inhibitors.
This sounds more complex than it is. Neurotransmitters send messages between cells. After the message is sent, the first cell “sucks it back up” like a sponge—this is called reuptake.
A reuptake inhibitor blocks this “sponge” action. This leaves more neurotransmitter in the space between cells, which can improve or strengthen communication between them.
Why the Difference Between SSRIs and SNRIs Matters
The key difference is that SSRIs affect only serotonin, while SNRIs affect both serotonin and norepinephrine. Serotonin helps regulate mood, sleep, and anxiety, while norepinephrine influences energy, alertness, and pain perception.
Because of this, SSRIs are often used for mood and anxiety disorders, whereas SNRIs may be more helpful when fatigue, low energy, or chronic pain are also present. One is not better than the other—the best choice depends on your symptoms, health, and how well you tolerate side effects.
SSRIs (Selective Serotonin Reuptake Inhibitors)
How They Work:
SSRIs block the reuptake of serotonin in the brain. (See call out box in introduction) This increases the amount of serotonin available in the synaptic space ( space between cells), which helps improve mood and reduce anxiety.
Why It Works:
Serotonin is a chemical messenger in the brain that helps the parts controlling mood, stress, sleep, and appetite work smoothly together. When there’s more serotonin between brain cells, messages pass more clearly, which can steady your mood, lower stress, reduce anxiety, and make you feel calmer and more positive.

Common SSRIs (ordered by U.S. market approval):
| Brand Name | Generic Name | How It Works | Notable Side Effect Tendencies |
| Prozac | Fluoxetine | Blocks serotonin reuptake; very long half-life (stays in body for days). Often energizing/activating. | Can cause insomnia, nervousness, mild nausea at start; less weight gain than others; lowest risk of withdrawal symptoms if stopped abruptly. |
| Zoloft | Sertraline | Blocks serotonin reuptake; also slightly affects dopamine reuptake at higher doses. | More GI upset early on (loose stools, nausea), mild insomnia; relatively low risk of weight gain. |
| Paxil | Paroxetine | Blocks serotonin reuptake; mild anticholinergic effects (dry mouth, sedation). Short half-life. | More sedating, higher risk of weight gain and sexual side effects, more intense withdrawal if stopped suddenly. |
| Luvox | Fluvoxamine | Blocks serotonin reuptake; has many drug interactions via liver enzymes (CYP450). Mostly used for OCD. | More sedating, more GI upset; needs careful management with other meds. |
| Celexa | Citalopram | Blocks serotonin reuptake; very “clean” except at high doses. | Well tolerated; at higher doses can prolong QT interval (heart rhythm), mild sexual dysfunction. |
| Lexapro | Escitalopram | Active isomer of citalopram; blocks serotonin reuptake with fewer interactions. | Considered one of the most “tolerable” SSRIs; mild nausea, headache, or insomnia; fewer side effects at therapeutic doses. |
Black Box Warning:**
All SSRIs carry an FDA black box warning for increased risk of suicidal thoughts and behaviors in children, adolescents, and young adults (under 25) during the first few months of treatment or dose changes.

SNRIs (Serotonin–Norepinephrine Reuptake Inhibitors)
How They Work:
SNRIs block the reuptake (see definition of reuptake in introduction) of both serotonin and norepinephrine. This increases the availability of these neurotransmitters in the brain.
Why It Works:
Both serotonin and norepinephrine exist in the spaces between brain cells—these spaces are called synapses. They act as chemical messengers, carrying signals from one cell (neuron) to another. When there’s more of either neurotransmitter in the synapse, the messages pass more efficiently, which strengthens their effects:
- Serotonin → steadies mood, lowers stress, supports sleep and appetite.
- Norepinephrine → boosts focus, alertness, energy, and readiness to respond to stress.

Common SNRIs (ordered by U.S. market approval):
| Brand Name | Generic Name | How It Works | Notable Side Effect Tendencies |
| Effexor XR | Venlafaxine (extended-release) | Blocks reuptake of serotonin (at low doses) and norepinephrine (at moderate/high doses). Short half-life. | May increase blood pressure at higher doses; can cause nausea, sweating, sexual dysfunction; strong withdrawal symptoms if stopped abruptly. |
| Cymbalta | Duloxetine | Blocks reuptake of serotonin and norepinephrine at all doses. Also FDA-approved for certain pain conditions. | Can cause nausea, dry mouth, constipation, fatigue, and increased sweating; less likely to raise blood pressure than venlafaxine. |
| Pristiq | Desvenlafaxine | Active metabolite of venlafaxine; similar action but steadier blood levels. | Side effects similar to venlafaxine but often fewer drug interactions; nausea and mild increase in blood pressure possible. |
| Fetzima | Levomilnacipran | Blocks reuptake of serotonin and norepinephrine; stronger norepinephrine effect than others. | More energizing; can increase heart rate and blood pressure; nausea, s |

Black Box Warning:**
All SNRIs also carry the same FDA black box warning for increased risk of suicidal thoughts and behaviors in children, adolescents, and young adults.
Key Differences Between SSRIs and SNRIs
| Feature | SSRIs | SNRIs |
| Neurotransmitters affected | Serotonin only | Serotonin + Norepinephrine |
| First approved (U.S.) | 1987 (Prozac) | 1993 (Effexor XR) |
| Typical use | Depression, anxiety, OCD, PTSD | Depression, anxiety, some chronic pain conditions |
| Energizing vs calming | Often more calming | Often more energizing (because of norepinephrine) |
| Blood pressure effects | Minimal | Possible increase (especially venlafaxine) |
Questions to Ask Your Doctor if Prescribed an SSRI or SNRI
- Why are you recommending this medication over others?
- How long will it take to notice improvements?
- What are the most common side effects I might experience?
- Will this medication affect my blood pressure, weight, or sleep?
- How will it interact with my other medications or supplements?
- How long should I stay on this medication once I feel better?
- How should I stop it if I need to discontinue (to avoid withdrawal symptoms)?
- Are there any warning signs (like worsening mood or suicidal thoughts) I should watch for?
- Does this medication have a black box warning, and what does it mean for me?
- Are there lifestyle changes or therapies that can make this medication work better?

Conclusion
SSRIs and SNRIs are antidepressants that boost brain chemicals between neurons. SSRIs focus on serotonin, while SNRIs boost both serotonin and norepinephrine, helping with depression, anxiety, and sometimes pain. Side effects are similar, and the right choice depends on your symptoms and medical history.
Addendum:
*Other antidepressants include MAO inhibitors and tricyclics, which can be effective but have more side effects.
**A black box warning is the FDA’s strictest alert, noting that SSRIs and SNRIs may increase suicidal thoughts in people under 25, especially early in treatment or with dose changes.
References / Citations
- National Institute of Mental Health. (n.d.). Depression. https://www.nimh.nih.gov/health/topics/depression
- U.S. Food & Drug Administration. (2023). Black box warnings and medication guides. https://www.fda.gov/drugs/drug-safety-and-availability/black-box-warnings
- Mayo Clinic. (2024). Antidepressants: Selecting one that’s right for you. https://www.mayoclinic.org/tests-procedures/antidepressants/about/pac-20384915
- National Alliance on Mental Illness. (n.d.). Mental health support and resources. https://www.nami.org/Home
- Mental Health America. (n.d.). Resources and tools for mental health. https://www.mhanational.org
- Find A Helpline. (n.d.). Directory of crisis helplines worldwide. https://findahelpline.com
- Stahl, S. M. (2021). Stahl’s essential psychopharmacology: Neuroscientific basis and practical applications (5th ed.). Cambridge University Press.
- Gelenberg, A. J., Freeman, M. P., Markowitz, J. C., et al. (2010). Practice guideline for the treatment of patients with major depressive disorder (3rd ed.). American Psychiatric Association. https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf
- Mayo Clinic Staff. (2024). SSRIs and SNRIs: How they work and what to expect. Mayo Clinic. https://www.mayoclinic.org/tests-procedures/antidepressants/about/pac-20384915
- MedlinePlus. (n.d.). Antidepressants. U.S. National Library of Medicine. https://medlineplus.gov/antidepressants.html